
The most common question I receive from those in the medical field, and those with heart conditions themselves, is, “What is your EF?” EF is an acronym for ejection fraction. In layman’s terms, the ejection fraction is simply calculated from the volume of blood being pumped into the heart and then ejected. This measures your pumping ability and determines your overall heart function. The following chart shows the diagnosis of your percentage.
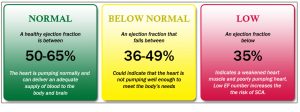
My current number is 34%. It is important to note that your ejection fraction changes constantly, somewhat like your blood pressure, as there are many variables to make it wobble some. The important issue is the trend in which your EF is heading. I have been diagnosed as high as 45% and as low as 21% in the past 8 years. I would also say that it depends on the testing used to determine the EF. An echocardiogram is the most commonly used diagnostic tool to determine EF, but is only reliable if the radiologist gets a good film and that the doctor reviewing the film, is any good at reading them. I have been told many times that my films are “hard reads” and so I am usually sent to have a MUGA scan or a cardiac MRI to substantiate my heart function. My last EF determination was calculated during a 3 hour MRI, so I am confident in that assessment. However, that was 8 months ago so who knows what it is currently. I will be getting another echo done shortly. Do not get fixated on your EF. I spent many years doing that and I always leave the office feeling duped. The appointments where I was sure that the EF had improved because I felt well, was able to exercise some, were always the lowest numbers. The appointments where I felt like getting out of bed was a monumental effort, those were the highest numbers. EF is a fickle bitch and she is just out to crush your expectations. Go with the flow on this. Just like receiving tattoos, (you know where people say the ribs hurt worse than the back. NOT FOR ME!) functionally we each respond differently to our EF. For example, some may not be able to walk across the room with an EF of 20%, but others are still working and functioning somewhat normally. I know from my own experience that I have felt like my functions were slower at a higher EF than I anticipated. It all just depends on what other heart ailments that are going on, your fluid retention at that time (salt must be limited) and your activity level. It is an entire “spa package” of delightfulness, with each “treatment” as intrinsic as the next in your “experience.”
Ok, so onward with my list of “deets” that I am currently experiencing. I am going to breeze through these in a bullet-like fashion without explanation of each. You can look up the details on your own if interested, or I can answer any questions in the comment section.
- Nonischemic Cardiomyopathy (Viral)
- Severe Heart Failure – 34%
- Ectopic Heartbeat – extra heartbeat
- Aortic Valve Regurgitation – Moderate
- Aortic Valve Sclerosis – Mild
- Pulmonary regurgitation – Mild
- Mitral Valve regurgitation – Mild
- Tricuspid Regurgitation – Mild
- Hypertrophic Cardiomyopathy – Left Ventricular Dysfunction
- Paroxysmal Supraventricular tachycardia
- Aortic Root Dilation
- Sleep Apnea – Moderate (contributes to heart failure)
I probably missed a few minor things, but you get the gist. My heart is a leaky basket case and pumps at the ability of an 80 year old. I should name her Estelle from Golden Girls. But, some would say, “You are not hospitalized or dying, just yet, so why the referral for a heart transplant?” My cardiologists have determined that there is nothing more they can do for me. I do not have a “smoking gun” such as a blockage that can alleviate my issues. In fact, I was told my heart arteries are “clean as a whistle.” I have damaged heart muscle, caused by a cold virus, which affects my ability to pump effectively (and the other items I listed which are secondary). Also, lets say they wanted to replace my aortic valve and that would mean a risky open-heart surgery. That procedure would only scratch the surface as to my overall problems. They want the fix to be a “one and done.”
The cardiologists have always scratched their heads on my specific diagnosis, and treating women with cardiac issues in general is something I could debate all day. I will spare you on that debate, but I will say that the doctors have always been quick to just point me in the direction of a heart transplant, as this is not my first referral for one. I am not sure if it means I am a hopeless case, or that they lack the experience and/or “give a shit” to reach further into their PHD’s to find me a cure. It could just be a liability thing as I was told by the first cardiologist I had, “Women like you scare me, because you die on me.” He wasn’t my cardiologist long after. All I know is I have been running away from the direction of heart transplant for years, but feel that my “opportunity slot” to do so, is narrowing. I guess the time is now. Anyway, there are more hoops to travel through than marrying your mother’s daughter on receiving a heart transplant. There are many people who are sick and the transplant centers only operate on a handful of them. The transplant center I am currently “dancing” with does approximately 55 a year; and hundreds are applying for them, such as me. The process to get approved for such a surgery is VERY long, ranging in diagnostic tests such as a heart biopsy (my big fear) to psychological evaluations on whether you will take care of your new heart properly. Also there are prerequisites: you have to be sick enough, but you cannot be too sick. That is the fine line in which I am currently hovering. You cannot have any other diseases or conditions. You can never have had cancer. You cannot be over the age of 65. You cannot have been a heavy drinker, smoker, drug abuser or criminal. There are also some restrictions on the disabled which I wont get into on this post, but I guarantee it will be something I post on later. Most importantly, you must have a high probability of success rate at recovery, as they don’t want the gift of donation to be wasted. The vetting process is rigid and I will post on it as I go along, if I even get accepted.
Although I am in the heart transplant evaluation stage, I would also like to explore the possibility of keeping my own heart and having a Left Ventricular Assist Device (LVAD).
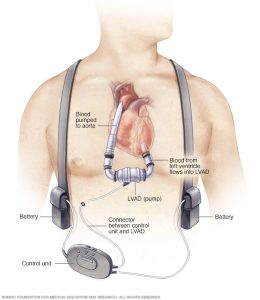
The LVAD is essentially a battery-operated mechanical pump that is implanted inside the chest to help a weakened left ventricle pump blood to the rest of the body. Unlike a total artificial heart, the LVAD does not replace the heart entirely, it is a bypass tube of the left ventricle. The weird thing is that you will not have a heart beat anymore. Some use this device as a bridge to heart transplant, and some use it as a temporary fix until the heart can heal again. Yes, some heart failure can heal, but after 8 years, I have been told mine will not. Then there are people like me who can use the LVAD as a permanent way to alleviate heart failure. It is a rough option; as you will carry battery-packs with you for life (approximately 15 years, which is the same longevity of a organ transplant). I would also find it difficult living in Florida and never swimming or taking a bath again as required, as the device has an external port in the abdomen to the battery packs and cannot get wet.
But there are just as many positives as negatives in the choice of an LVAD, and all the choices we make in this journey. Let’s get one thing out there though, none of the choices are particularly good or exciting ones, but it is those choices or a slow demise. We each will have to choose inaction, or action. Your life situation is the best way to do that, as I feel if I didn’t have children that my choices would be different. But I do have children who still need me, so I must act. I must teach them that when life gives you a struggle, that you meet it; chest puffed out and with determination to win. And if I cannot win, I must show them how to be brave in the face of it – even if I am scared shitless. As a mother, I know what it is like to teach my kids to live, and so I believe that if that time comes, I must also teach them how to die; with dignity, with their sword bloody and with a gleam in their eye. I have no idea how to do this yet, but it has become my new aspiration. Ok, this just went deeper than I intended. Enough for today, I think.